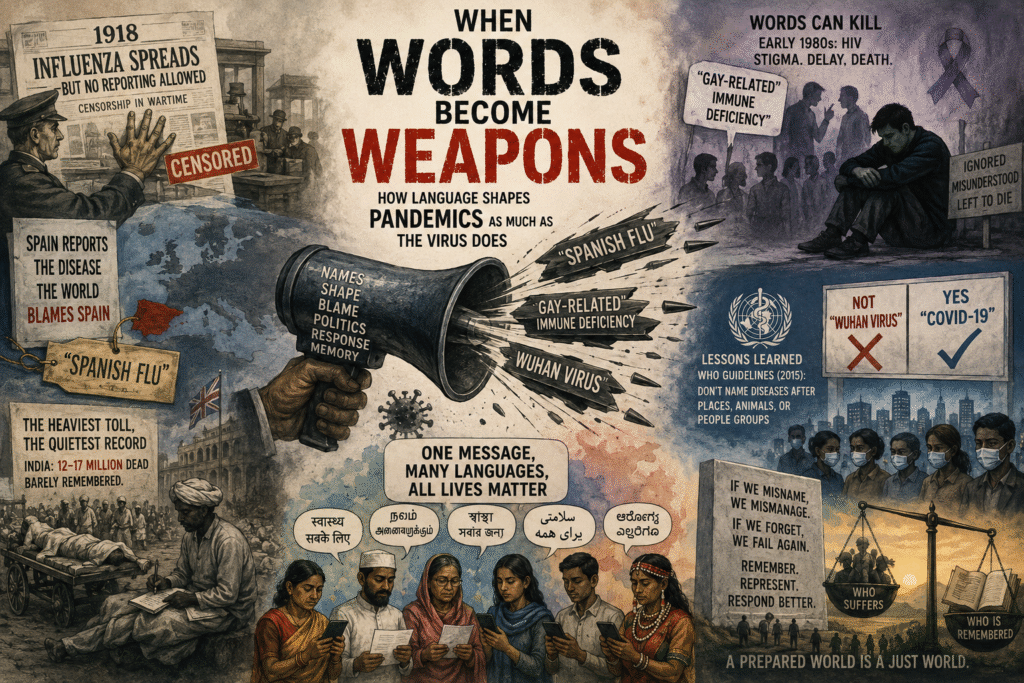
Pandemics are not just biological crises — how naming, blame, and language determine who survives and who is forgotten. Pandemics leave behind not only biological scars but linguistic and political ones that shape memory, blame, and survival.
Every pandemic leaves two bodies of evidence behind: the biological and the cultural. We have grown reasonably adept at cataloguing the first — mortality curves, transmission rates, variant genealogies. The second, which shapes how societies respond, whom they blame, and how long they remember, receives far less rigorous attention.
Science journalist Laura Spinney, author of Pale Rider: The Spanish Flu of 1918 and How it Changed the World, is among a small number of thinkers working to change that. Her argument, laid out in a recent episode of the WHO’s Global Health Matters podcast, is disarmingly simple: a pandemic’s impact is shaped as much by human behaviour and language as by the pathogen itself.
That argument deserves a long look.
The forgotten pandemic
The 1918 influenza pandemic was, by most epidemiological measures, the deadliest infectious disease event in recorded human history. Estimates of the global death toll range from 50 million to 100 million — a figure that dwarfs the First World War being fought simultaneously.
Yet, as Spinney notes, it sits curiously absent from collective memory. Most people can name the assassination of Archduke Franz Ferdinand; very few can name where the 1918 flu first appeared or how it ended.
Part of the amnesia is structural. The pandemic unfolded across a period of censorship — warring governments suppressed early reporting to preserve public morale. Spain, neutral in the conflict and therefore free to report, became the visible face of an illness it did not cause. The name “Spanish flu” stuck, and with it came a misremembering that has persisted for over a century.
Part of the amnesia is also geographical. Popular histories of the 1918 pandemic remain anchored in Europe and North America, where archives are richest and historians most numerous. In fact, the pandemic’s most catastrophic toll fell on the colonised world.
India, then under British imperial administration, lost somewhere between 12 and 17 million people — a figure larger than the entire military death toll of the First World War. Those deaths barely register in the conventional pandemic narrative. The communities that bore the greatest burden were least equipped to document their suffering, and the world’s memory reflects that asymmetry.
Why naming matters
Spinney’s most pointed intervention concerns language, specifically the act of naming an outbreak. When a novel pathogen emerges, it requires a name almost immediately — not for bureaucratic tidiness, but because, as she observes, you cannot respond to something you cannot talk about.
A name enables surveillance systems, clinical protocols, public health messaging, and political decisions to cohere around a shared object.
But names do not merely describe. They assign. They locate. They implicate.
“Spanish flu” located blame in a country that was a victim rather than a source. The label survived because it was convenient and because Spain lacked the geopolitical leverage to challenge it.
The downstream consequences were real: misattribution of origin delayed coherent international response and seeded resentments that fed into post-war political instability.
The pattern is not unique to 1918. When HIV emerged in the early 1980s, it was initially categorised as a “gay-related immune deficiency”. That framing was catastrophic.
It channelled stigma, distorted research priorities, delayed mainstream public health intervention, and condemned thousands to death who might otherwise have received earlier care. The label was scientifically inaccurate — HIV was a bloodborne pathogen with no intrinsic relationship to sexual orientation — but once attached, it proved extraordinarily resistant to correction.
The World Health Organisation absorbed this lesson, at least formally. In 2015 it issued guidelines discouraging the naming of diseases after places, animals, or population groups, precisely to prevent the stigma and economic harm that such names inflict.
“COVID-19” rather than “Wuhan virus” was a deliberate application of those guidelines. Whether the guidelines hold under political pressure — as the current era amply demonstrates — is another matter.
The multilingual challenge
Spinney raises a second, less-discussed dimension: the linguistic structure of global health governance itself. International health discourse is conducted overwhelmingly in English.
Epidemiological data, WHO guidance, clinical trial results, and media coverage flow through a single linguistic channel. In a public health emergency, this creates a fundamental inequality.
Communities whose primary languages are not English receive translated information — when they receive it at all — more slowly, with greater risk of distortion, and with less ability to push back against framings that do not match their lived reality.
This matters enormously for a country like India, which navigates over 20 constitutionally recognised languages and hundreds more in everyday use.
During COVID-19, the gap between English-language public health communication and vernacular comprehension was not merely an inconvenience; it shaped compliance, vaccine uptake, and mortality in measurable ways.
Spinney’s call for a more inclusive linguistic approach to global health is not an abstract diversity argument. It is a practical epidemiological one.
The 1918 flu as mirror
What makes Spinney’s work valuable is that it treats the 1918 pandemic not as a historical curiosity but as a diagnostic tool.
The pandemic, she argues, accelerated the first half of the twentieth century. It weakened European imperial powers at a moment when colonised nations were already straining toward independence.
It shaped the terms of the Paris Peace Conference of 1919 — Woodrow Wilson’s negotiating capacity was reportedly compromised by a severe influenza attack during the talks.
It influenced modernist art and literature, which grappled with mass death, bodily vulnerability, and the limits of rational progress. It contributed to the conditions that produced the Great Depression and, eventually, the Second World War.
None of these connections are linear or deterministic. But dismissing the 1918 flu as merely a public health event obscures how deeply biological crises knit themselves into political, economic, and cultural life.
The pandemic did not happen to history; it was part of it.
What this means for preparedness
The current global conversation on pandemic preparedness — shaped by the post-COVID reckoning and ongoing negotiations around the WHO Pandemic Accord — focuses heavily on vaccines, surveillance systems, and pathogen-sharing agreements.
These are essential. But Spinney’s framework suggests that preparedness must also encompass the social sciences: how communities understand risk, how naming decisions are made and contested, how health communication reaches populations in their own languages, and how accountability is assigned when crises cross borders.
A pandemic that is misnamed from the start will be mismanaged from the start. A response conducted only in one language will save only some lives. And a recovery that forgets who suffered most will lay the foundations for the next catastrophe.
The virus, it turns out, is the simpler part of the problem.